Surgery Case Sheet Presentation
| Introduction to Surgery Case Sheet | ||
|---|---|---|
| A surgery case sheet is a document used to record all relevant information about a surgical procedure. It serves as a comprehensive record for the surgical team and other healthcare providers involved in the patient's care. The case sheet includes important details such as patient demographics, medical history, surgical plan, and post-operative care instructions. | ||
| 1 | ||

| Importance of Surgery Case Sheet | ||
|---|---|---|
| A well-documented surgery case sheet ensures accurate and efficient communication among healthcare providers. It helps in tracking the patient's progress throughout the surgical process and assists in making informed decisions. The case sheet serves as a legal document, providing evidence of the surgical procedure and the care provided. | ||
| 2 | ||
| Contents of a Surgery Case Sheet | ||
|---|---|---|
| Patient demographics: Includes the patient's name, age, gender, contact information, and identification number. Medical history: Records the patient's past and current medical conditions, allergies, medications, and previous surgeries. Pre-operative assessment: Documents the results of pre-operative tests, physical examination, and anesthesia evaluation. | ||
| 3 | ||
| Contents of a Surgery Case Sheet (continued) | ||
|---|---|---|
| Surgical plan: Describes the planned procedure, including the surgical approach, anticipated complications, and special equipment required. Intra-operative details: Records the start and end time of the surgery, surgical team members involved, and any unexpected events or complications. Post-operative care: Outlines the instructions for wound care, pain management, activity restrictions, and follow-up appointments. | ||
| 4 | ||
| Documentation of Anesthesia | ||
|---|---|---|
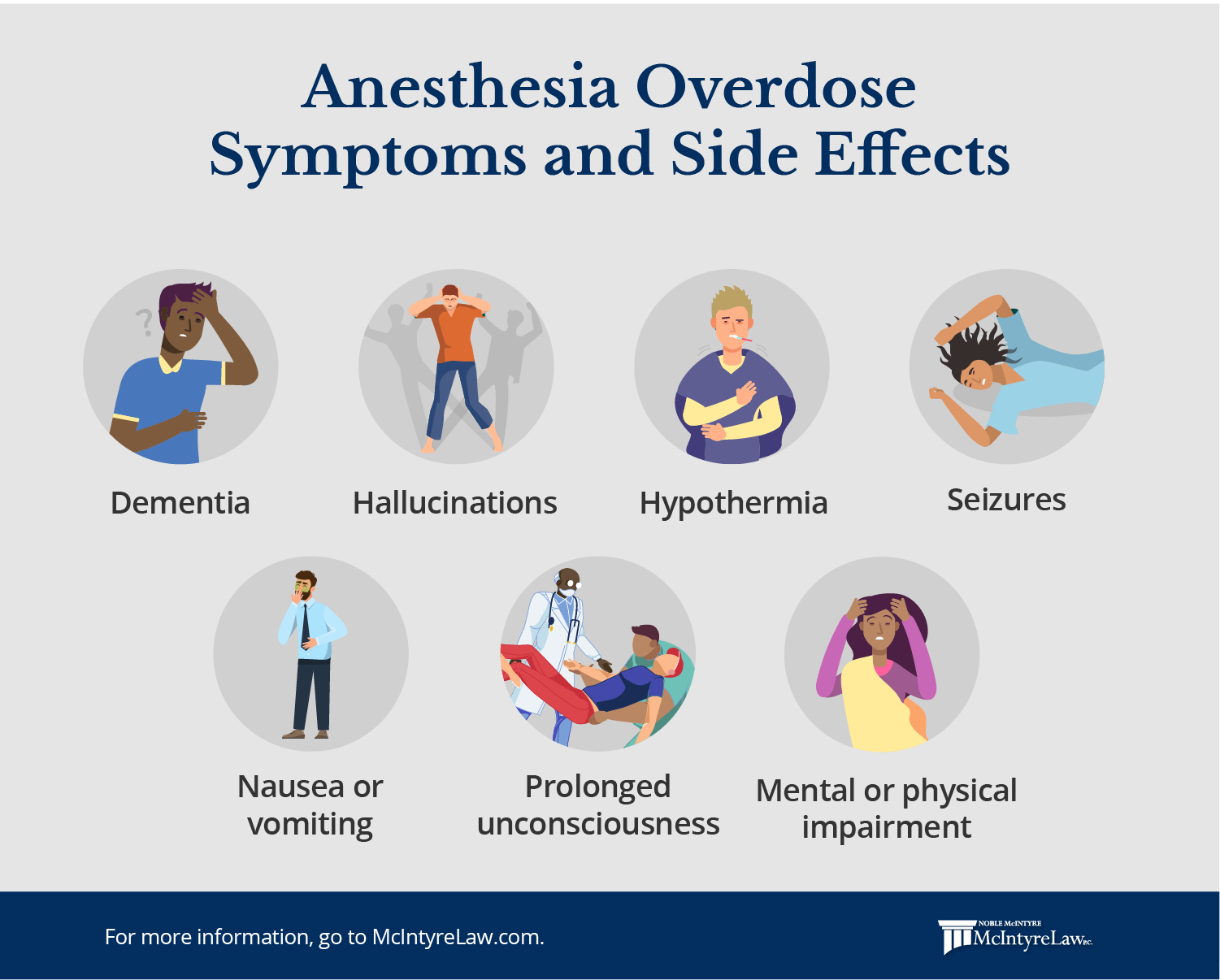
| Anesthesia details: Includes the type of anesthesia used, the dose administered, and any adverse reactions or complications during anesthesia. Vital signs: Records the patient's blood pressure, heart rate, oxygen saturation, and temperature throughout the surgery. Anesthetic medications: Documents the drugs administered during anesthesia, including their doses and any adverse effects. | ||
| 5 | ||
| Surgical Instrumentation and Materials | ||
|---|---|---|
| Instrument count: Verifies the number of instruments used before and after the surgery to ensure no items are left inside the patient. Implants and prosthesis: Includes details of any artificial devices or materials used during the procedure, such as implants or joint replacements. Blood and fluid management: Records the amount of blood loss, fluid replacement, and any transfusions during the surgery. | ||
| 6 | ||

| Complications and Follow-up | ||
|---|---|---|
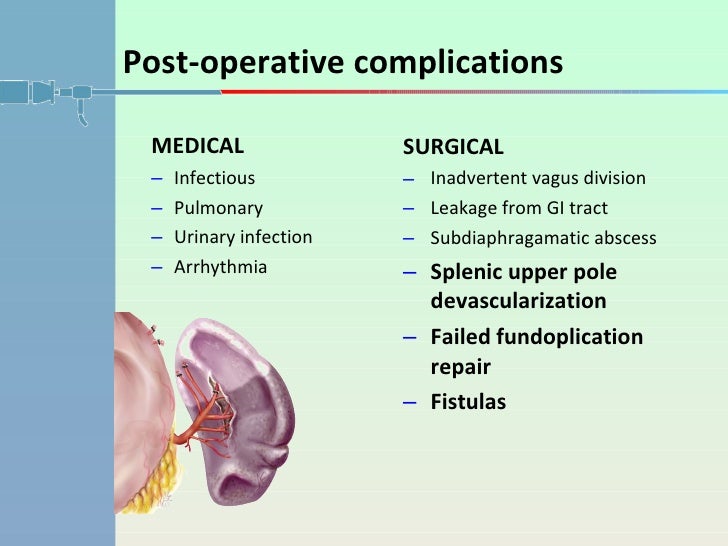
| Intra-operative complications: Documents any unexpected events, complications, or conversions to a different surgical procedure. Post-operative complications: Records any complications that arise after the surgery, such as infection, bleeding, or wound dehiscence. Follow-up instructions: Provides guidance on post-operative care, medication regimen, and scheduled follow-up visits. | ||
| 7 | ||
| Signatures and Amendments | ||
|---|---|---|
| Surgeon's signature: Confirms the completion of the surgical procedure and assumes responsibility for the patient's care. Anesthesiologist's signature: Verifies the administration of anesthesia and the patient's safe recovery from anesthesia. Amendments: Any updates or changes to the case sheet should be clearly documented with the date, time, and initials of the healthcare provider. | ||
| 8 | ||

| Storage and Confidentiality | ||
|---|---|---|
| Storage: Case sheets should be stored securely to ensure confidentiality and easy retrieval when needed for reference or legal purposes. Accessibility: Authorized healthcare providers should have access to the case sheets to facilitate continuity of care. Confidentiality: Patient privacy and confidentiality should be maintained at all times, following healthcare regulations and guidelines. | ||
| 9 | ||

| Summary and Conclusion | ||
|---|---|---|
| A well-prepared and comprehensive surgery case sheet is crucial for effective communication, patient safety, and legal documentation. It serves as a reference for healthcare providers involved in the patient's care and facilitates continuity of care. Strict adherence to documentation standards, storage, and confidentiality is essential to ensure the integrity and privacy of the case sheets. | ||
| 10 | ||
